Obstetrics and Gynecology
A branch of medicine that specializes in the care of women during pregnancy and childbirth and in the diagnosis and treatment of diseases of the female reproductive organs.
Who is a Gynecologist?
A specialist that deals with women’s health and reproductive organs including the uterus, ovaries, fallopian tubes, cervix, and vagina. Gynecologists diagnose and treat conditions such as menstrual disorders, pelvic pain, infertility, and menopause-related concerns.
Who is an Obstetrician?
A specialist that deals with pregnancy and childbirth.
Common Conditions that are treated by an Obs/Gynae are:
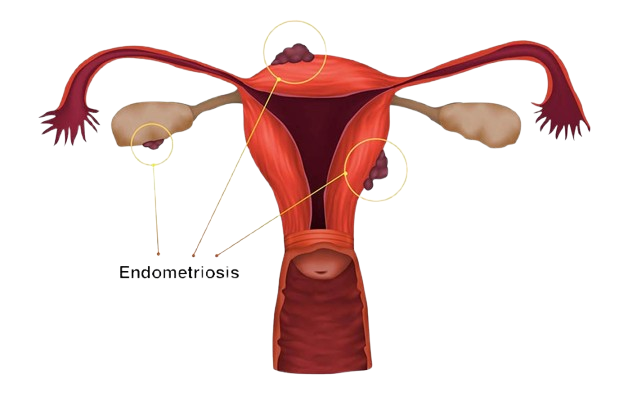
- Endometriosis
- Ovarian Cysts
- Ectopic Pregnancy
- Unexplained Infertility
- Pelvic Adhesions
- Uterine Polyps (Endometrial Polyps)
- Uterine Fibroids (Leiomyomas or Myomas)
- Uterine Septum or Intrauterine Adhesions
- Intrauterine Adhesions (Asherman’s Syndrome)
- Abnormal Uterine Bleeding (AUB)
Procedures for the Treatment of Above Conditions
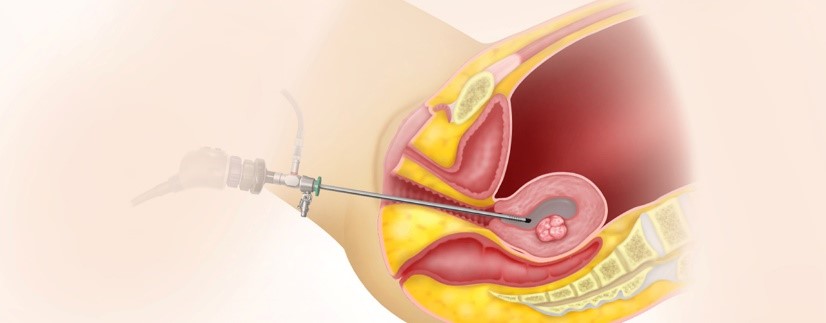
1. Laparoscopy
Small incisions are made in the abdomen to insert a camera and instruments.
Used to diagnose or treat:
Endometriosis
Endometriosis is a condition where tissue similar to the uterine lining grows outside the uterus — commonly on the ovaries, fallopian tubes, or pelvic lining. This tissue continues to thicken, break down, and bleed with each menstrual cycle, causing inflammation and scar tissue.
Symptoms May Include:
- Severe pelvic pain (especially during periods)
- Pain during intercourse
- Heavy menstrual bleeding
- Infertility
How We Help:
- Pelvic exam and imaging (ultrasound, laparoscopy)
- Pain relief and hormonal treatments
- Laparoscopic surgery to remove or destroy endometrial implants
- Fertility planning if conception is a concern
Ovarian Cysts
Ovarian cysts are fluid-filled sacs that develop on or inside an ovary. Most are harmless and resolve on their own, but some may grow large, rupture, or cause complications.
Symptoms May Include:
- Bloating or abdominal swelling
- Pelvic pain (especially on one side)
- Menstrual irregularities
- Pain during intercourse or bowel movements
How We Help:
- Diagnosis via pelvic ultrasound
- Monitoring of functional cysts
- Hormonal birth control to prevent future cysts
- Laparoscopic surgery (cystectomy) if the cyst is large, persistent, or painful
Ectopic Pregnancy
An ectopic pregnancy occurs when a fertilized egg implants outside the uterus, most often in a fallopian tube. This is a life-threatening emergency and must be treated promptly.
Symptoms May Include:
- Sharp pelvic or abdominal pain
- Vaginal bleeding
- Shoulder pain
- Dizziness or fainting (signs of rupture)
How We Help:
- Urgent diagnosis with ultrasound and blood tests
- Medical management with methotrexate (if early and unruptured)
- Surgical intervention (laparoscopic or open) if ruptured
- Emotional support and follow-up care
Pelvic Adhesions
Pelvic adhesions are bands of scar tissue that cause organs in the pelvis to stick together. They often develop after surgery, infection, endometriosis, or injury.
Symptoms May Include:
- Chronic pelvic pain
- Pain during intercourse or bowel movements
- Infertility
How We Help:
- Diagnosis via laparoscopy (often the only definitive method)
- Adhesiolysis (surgical removal of adhesions)
- Fertility assessment and treatment planning
Unexplained Infertility
Unexplained infertility is diagnosed when a couple is unable to conceive despite normal test results for ovulation, sperm quality, fallopian tube patency, and uterine health.
We Investigate and Support Through:
- Hormonal evaluations
- Ovulation tracking and cycle monitoring
- Imaging tests (HSG, ultrasound)
- Laparoscopy to rule out hidden endometriosis or adhesions
- Fertility treatments (ovulation induction, IUI referrals, IVF coordination)
2. Hysteroscopy
- A thin scope is inserted through the cervix into the uterus.
- Used to diagnose and treat:
Uterine Polyps (Endometrial Polyps):
Uterine polyps are soft, non-cancerous growths attached to the inner lining of the uterus (endometrium). They vary in size and can cause abnormal bleeding or fertility issues.
Symptoms May Include:
- Irregular or heavy menstrual bleeding
- Bleeding between periods
- Postmenopausal bleeding
- Difficulty getting pregnant
How We Treat:
- Diagnosis via transvaginal ultrasound or hysteroscopy
- Removal using hysteroscopic surgery (minimally invasive)
- Pathology testing to rule out pre-cancer or cancer
Uterine Fibroids (Leiomyomas or Myomas)
Fibroids are non-cancerous tumors made of muscle and connective tissue that grow in or on the uterus. Their size and location determine symptoms and treatment needs.
Symptoms May Include:
- Heavy or prolonged periods
- Pelvic pressure or pain
- Frequent urination or constipation
- Infertility or miscarriage
How We Treat:
- Monitoring (if asymptomatic)
- Medication to manage symptoms (hormonal therapy)
- Minimally invasive removal (myomectomy)
- Uterine fibroid embolization (UFE)
- Hysterectomy (in severe or refractory cases)
Uterine Septum / Intrauterine Adhesions
A congenital abnormality where a wall of tissue (septum) divides the uterus partially or completely. It’s a common cause of recurrent miscarriage or infertility.
How We Treat:
- Diagnosis via 3D ultrasound or MRI
- Hysteroscopic septum resection — a minimally invasive surgery to remove the dividing tissue
Intrauterine Adhesions (Asherman’s Syndrome)
Scar tissue that forms inside the uterus, often after a D&C procedure, infection, or previous uterine surgery. It can lead to menstrual irregularities or infertility.
Symptoms May Include:
- Light or absent periods
- Infertility
- Recurrent miscarriage
How We Treat:
- Hysteroscopy to remove adhesions
- Hormone therapy to promote healing of the uterine lining
- Ongoing monitoring of menstrual cycles and fertility
Abnormal Uterine Bleeding (AUB)
Any bleeding that differs from your normal menstrual cycle, including:
- Heavy or prolonged periods
- Bleeding between periods
- Bleeding after intercourse
- Postmenopausal bleeding
Causes May Include:
- Hormonal imbalances
- Fibroids or polyps
- Endometrial hyperplasia or cancer
- Thyroid disorders, PCOS, or clotting issues
How We Treat:
- Hormonal treatments (birth control, IUDs, medications)
- D&C (dilation and curettage) for diagnosis and treatment
- Hysteroscopy to evaluate the uterus
- Surgical options if needed (e.g., endometrial ablation, fibroid removal)
Major Surgical Procedures
1. Hysterectomy
Partial (supracervical): Removes the uterus but leaves the cervix
Total hysterectomy: Removes both uterus and cervix
Radical hysterectomy: Also includes surrounding tissues and part of the vagina (usually for cancer)
Can be done via:
- Abdominal surgery
- Vaginal surgery
- Laparoscopic or robotic-assisted techniques
2. Myomectomy
Surgical removal of fibroids while preserving the uterus. Ideal for women who wish to retain fertility.
3. Oophorectomy / Salpingo-oophorectomy
Removal of one or both ovaries and/or fallopian tubes. Used in cases of cysts, cancer, or risk reduction (e.g., BRCA mutation).
4. Cystectomy
Removal of ovarian cysts while preserving the ovary if possible.
5. Tubal Ligation
Permanent sterilization procedure.
Fallopian tubes are cut, tied, or sealed to prevent pregnancy.
Pre-Procedure Instructions
For Pap Smear / Colposcopy:
- Avoid intercourse, douching, or using vaginal medications for 48 hours prior.
- Schedule the test when you’re not on your period.
- Wear comfortable clothes.
For Ultrasound (Pelvic or Transvaginal):
- Pelvic ultrasound: Come with a full bladder (drink water 1 hour before).
- Transvaginal ultrasound: Empty your bladder before the scan.
- No fasting is required.
For Minor Surgery (IUD insertion, biopsy, etc.):
- Eat a light meal before the procedure.
- Take an over-the-counter pain reliever (e.g., ibuprofen) 30–60 minutes prior if advised.
- Arrange for someone to drive you home if sedatives are used.
For Major Surgery (Laparoscopy, Hysterectomy):
- Do not eat or drink after midnight the night before surgery.
- Stop certain medications (blood thinners, supplements) as advised.
- Arrange for help at home during recovery.
- Bring all relevant medical records, test results, and consent forms.
Diagnostic Procedures
1. Pelvic Exam
A routine procedure to examine the external and internal reproductive organs. Often includes:
- Visual inspection of the vulva
- Speculum exam to view the cervix
- Bimanual exam to feel the uterus and ovaries
2. Pap Smear (Pap Test)
A screening test for cervical cancer that involves collecting cells from the cervix. Often combined with HPV testing.
3. Colposcopy
Used when a Pap smear shows abnormal results. A special magnifying device is used to examine the cervix, vagina, and vulva. May include biopsy of suspicious areas.
4. Endometrial Biopsy
A sample of the uterine lining (endometrium) is collected. Commonly used to evaluate abnormal uterine bleeding, postmenopausal bleeding, or suspected endometrial cancer.
5. Transvaginal Ultrasound
An internal ultrasound using a probe inserted into the vagina. Provides high-resolution images of the uterus, ovaries, and fallopian tubes. Commonly used for pelvic pain, infertility, and early pregnancy assessment.
Non-Surgical Treatments

- IUD Insertion/Removal: Long-acting reversible contraception (hormonal or copper). A quick outpatient procedure.
- Nexplanon Insertion/Removal: A small rod placed under the skin of the arm that releases hormones for birth control.
- Bartholin Cyst Drainage: Treats infected or swollen Bartholin glands near the vaginal opening.
- Cryotherapy: Freezing abnormal cervical tissue (often used for treating cervical dysplasia or warts).
Post-Procedure Care Instructions
After Colposcopy / Biopsy:
- Expect light spotting or discharge for 1–3 days.
- Avoid tampons, swimming, or sex for about a week, or as advised.
After Laparoscopy:
- You may have mild shoulder pain (from gas used during surgery).
- Limit physical activity for 1–2 weeks.
- Keep the incisions clean and dry. Watch for signs of infection (redness, swelling, fever).
After Hysterectomy:
- Recovery typically takes 4–6 weeks.
- No intercourse, heavy lifting, or baths during this time.
- Light walking is encouraged to prevent blood clots.
Frequently Asked Questions (FAQs)
What is the difference between a gynecologist and an obstetrician?
A gynecologist specializes in the female reproductive system and women's health, while an obstetrician cares for pregnant women, delivers babies, and handles postnatal care. Most OB/GYNs are trained in both.
How often should I have a Pap smear?
Women between ages 21–65 should have a Pap smear every 3–5 years, depending on their age, risk factors, and previous results. Your doctor will recommend what’s right for you.
What should I expect during my first gynecological exam?
Your first visit may include a general physical exam, pelvic exam, breast check, and discussion about your medical and menstrual history. It’s a great time to ask questions about periods, birth control, or sexual health.
Is it normal to feel discomfort after an IUD insertion?
Yes, mild cramping and spotting are common for a few days. Severe pain or heavy bleeding, however, should be reported immediately.
Can I still get pregnant after a fibroid removal (myomectomy)?
Yes. Myomectomy removes fibroids while preserving the uterus, and many women conceive afterward. Your doctor will guide you on the ideal timing for pregnancy post-surgery.
Is laparoscopic surgery safe?
Yes. It’s a minimally invasive technique with fewer complications, quicker recovery, and less pain compared to open surgery.